

Summary
This review paper provides an overview of basic knowledge on essential fatty acids and their effect on early brain development. Special attention is given to the importance of omega–3 fatty acids – docosahexaenoic and eicosapentaenoic acid – in brain structure and functioning, as well as the importance of an optimal intake of these nutrients during pregnancy and early childhood.
Key words: early brain development, essential fatty acids
Numerous scholarly sources examine the influence of food on the process of child growth and development, and in overcoming health problems and intellectual development impairments. Studies on the effects of unsaturated fatty acids in the maternal and infant diet on early brain development seem particularly interesting. Compared to other organs, the brain contains the highest concentration of fat. Phospholipids make up almost two thirds of its weight. Phospholipids consist of two glycerol molecules, which bind two fatty acid molecules and one phosphate consisting of a single organic molecule (e.g. choline) to their hydroxyl group [1]. Phospholipids form bilayer structures and play an important role in building cell membranes.
Essential fatty acids (EFA) are unsaturated fatty acids with two or more double bonds in the molecule. They are also called long-chain polyunsaturated fatty acids (LCPUFA). They are necessary for maintaining optimal health, but cannot be synthesised within the body, which means they have to be introduced into the body with food. They retain their liquid form even in cold water. There are two groups of LCPUFA: omega-6 (linoleic) and omega-3 (alpha-linolenic) fatty acids [2, 3]. The adult human body metabolises them into long-chain fatty acids via desaturation, which creates a new double bond at the molecule’s carboxylic end. Omega-6 acids (LA) are transformed into gama-linolenic acid (GLA) and then – through further desaturation – into arachidonic acid (AA). The process of desaturisation turns omega-3 polyunsaturated fatty acid (alpha linolenic acid; ALA) into eicosapentaenoic (EPA), then docosapentaenoic (DPA) and finally docosahexaenoic (DHA) acid [4, 5]. The brain contains the largest concentration of DHA, which is mostly distributed in the cerebral cortex, mitochondria and the photoreceptors in the retina [6]. DHA encompasses around 40% of long-chain polyunsaturated fatty acids (LCPUFA) in the brain and 60% in the retina. It makes up almost 50% of the neurone membrane weight. Other fatty acids – arachidonic (AA) and eicosapentaenoic (EPA) acid – play an important role in brain cell development and functions. Like other useful micronutrients – vitamin B complex, vitamin C, vitamin E, iodine, iron, zinc, copper, taurine, choline, etc. – they are crucial for brain development, integrity and function [7]. LCPUFA are an important dietary source of energy. When taken in the recommended amounts – ranging from 5–10:1 to 1:3.4 (the ratio found in breast milk) – omega-6 and omega-3 fatty acids play a key role in maintaining the structural and functional integrity of the central nervous system. Omega-6 fatty acids also stimulate thrombocyte inflammation and aggregation. Omega-3 fatty acids have anti-inflammation traits and prevent thrombocyte accumulation. The omega-6 fatty acid metabolism includes the production of numerous eicosanoids (such as thromboxane, leukotriene and prostaglandine), which cause inflammation and atherosclerosis [8]. The final product of omega-6 fatty acid desaturation, arachidonic acid, is the most powerful inflammation agent. It stimulates the production of glutamate, a neurotransmitter which triggers neuron destruction, thus causing the hyperproduction of free oxygen radicals. In contrast, omega-3 fatty acids and DHA reduce cellular and vascular brain inflammations, and ensure brain cell membrane integrity. DHA reduces the level of thromboxane and increases tissue perfusion and oxygen distribution by expanding the blood vessels and reducing blood viscosity. Some reports suggest that DHA neutralises free radicals and increases levels of serotonin (neurotransmitters that make us “feel good”) and acetylcholine (“improved memory”) [9].
During pregnancy, the foetus is completely dependent on maternal DHA sources from lipid supplies, derived from the maternal diet and food supplements. The placenta actively and selectively transmits AA and DHA from the maternal into the foetal blood stream. The foetus’ ability to transform ALA to DHA is limited [9]. During the third trimester of the pregnancy, there is ample DHA accumulation in the liver, brain and retina of the foetus [10]. During pregnancy, DHA is progressively drawn from the mother’s plasma, possibly due to the increased accumulation of this key nutrient in the developing neural system [11]. The final trimester is the period of the most rapid brain development, so DHA requirements are higher than in any other period of human life. Maternal supplies are therefore gradually (sometimes never fully) recovered during a 5- to 6-month period following delivery (Fig. 1, according to [12]).
There is evidence to support the existence of an important link between emptying DHA supplies in the maternal blood and depression during and after pregnancy. In infancy, breast milk provides sufficient amounts of DHA to meet the child’s requirements. Human milk contains 30 times more DHA than the milk of other mammals. This amount can be further increased by introducing appropriate food supplements to the breastfeeding mother’s diet [7]. There is a linear correlation between the amount of DHA in the breastfeeding woman’s diet and the amount of DHA in her breast milk [13,14]. Low EFA levels in children are the result of insufficient EFA intake, reduced transformation of LA and ALA into longer and more unsaturated fatty acids, and enhanced LCPUFA metabolism [15].
Effects of LCPUFA on brain development
Prematurely born infants are especially sensitive to EFA deficiency, created through a lack of adipose tissue at birth, possible fatty acid metabolism immaturity (elongation/desaturation) or insufficient levels of ALA and DHA in infant food [16]. In previous decades, several studies examined the influence of LCPUFA on the lipid system in the plasma and tissue, the retinal electro-physiological function and the maturation of the visual cortext. The research encompassed breast- and formula-fed infants (one group feeding on standard infant formula and the other on formula supplemented with omega-3 fatty acid). The Teller card and SWEEP-VEP testing (swept visual evoked potentials; type of VEP which measures vision acuity based on structural eye stimulus) measured the highest results among infants who were breastfed at the age of 2 and 4 months. The results of SWEEP-VEP testing reveal noticeable differences at the age of 2 and 4 months: infants fed by LCPUFA-supplemented formula had higher results than infants feeding on non-LCPUFA-supplemented formula [17].
Compared to formula-fed infants, breastfed infants show better progress in terms of cognitive development. The length of breastfeeding has a positive correlation to adult IQ [17]. The differences predicated on diet and cognitive development disappear after 9 months of breastfeeding [18]. Comparisons of term and prematurely born infants’ diets suggest that breastfed prematurely born infants show greater progress when it comes to intelligence development than infants with normal birth weight breastfed for the same amount of time [19]. The same study suggests that beneficial effects of breastfeeding are prominent among prematurely born infants, compared to term infants. It is worth noting that, due to a number of accompanying socio-emotional influences, these effects cannot be exclusively linked to nutritive factors.
Direct benefits of LCPUFA-supplemented formula were observed. One double-blind experiment studied healthy term infants fed by LCPUFA-supplemented formula and plain infant formula during the first 2 months. Measurements of general spontaneous movement quality which bear witness to the child’s neuromotor development were conducted at the age of 3 months. The group of infants fed by LCPUFA-supplemented-formula had significantly better results compared to infants fed on plain infant formula [21].
Beneficial effects were identified among mothers taking LCPUFA supplements during pregnancy. At the age 2.5 years, the development of their children was measured on the Griffiths Mental Development Scales. These children showed greater progress in terms of coordination than the children whose mothers had not consumed LCPUFA supplements during pregnancy. Another group of children whose mothers took DHA supplements during pregnancy achieved significantly higher results compared to the control group, when assessed by the Bayley Scales of Infant Development – Psychomotor Development Index [22]. The authors of this study warn that literature on the effects of LCPUFA supplements still contains a significant amount of controversial information.
LA and AA deficiency causes skin dryness and thinning (accompanied by skin peeling and intertrigo) as well as growth, body mass index and metabolism increment disorders [23]. There is a significant negative correlation between the LA percentage in the phospholipids of the foetal plasma and head circumference. Maternal LA consumption in the mid pregnancy period stands in negative correlation to neonatal head circumference [24]. Head circumference is an important indicator of brain weight, while AA and DHA present the main “building blocks” of the brain [25]. Increased maternal LA consumption and a smaller head circumference may perhaps be explained by reference to excessive LA availability, which leads to the inhibition of desaturation substrates, which is necessary for EFA to be properly turned into LCPUFA. Furthermore, it has been proven that LA prevents LCPUFA from mixing inside the plasma and entering tissues [26], which suggests that the ratio between omega-3 and omega-6 PUFA in the current diet is too low and needs to be regulated, ideally by substituting ALA with LA [27]. Some studies of problematic pregnancies show that taking LCPUFA supplements reduces the risk of premature delivery. This type of therapy has not been proven to increase the infant’s birth weight or reduce the risk of preeclampsia [28, 29].
One study of the possible influences of DHA supplements administered to breastfeeding mothers observed two groups of children below the age of 5 years: 1) infants whose mothers took DHA supplements during breastfeeding; and 2) infants whose mothers took placebo. No significant differences in visual functions were determined (Bailey-Lovie chart and VEP). Attentional abilities were measured on the Leiter International Performance Scales; no statistically relevant differences between the two groups were found. Infants whose mothers consumed DHA had better results in tests of continuous attention, which suggests that these infants enjoy long-term benefits in specific neuropsychological domains [30].
Some studies have proven that children suffering from ADHD have significantly lower EFA blood levels [15, 31, 32]. Children suffering from ADHD (attention-deficit/hyperactivity disorder) are unfocused, impulsive and hyperactive [15]. Studies have shown that these children have lower fatty acid concentrations in the polar lipids in the plasma, as well as lower fatty acid concentrations in the erythrocyte membranes (mostly AA, EPA and DHA [31]). It has been indicated that children with ADHD have not been breastfed at all or have been breastfed for a short period of time (shorter than children in control groups [15, 31]). Another study conducted among persons with ADHD focused on their somatic problems, such as excessive thirst, frequent urination, dry skin, dry hair, follicular keratosis, dandruff, brittle nails, asthma and/or frequent ear inflammations. Research subjects with more pronounced symptoms had significantly lower levels of AA and DHA in the plasma compared to those with less frequent symptoms. Based on these characteristics, this group was defined as L-ADHD, and the group of symptoms termed EFA deficiency symptoms [31]. Furthermore, children suffering from ADHD and receiving medicamentous treatment with methylphenidate or pemoline have higher omega-3 fatty acid levels in the plasma and erythrocyte membranes [31]. When considering total omega-3 concentration in comparison to total omega-6 concentration in plasmatic lipids, it has been concluded that children with lower n-6 levels – regardless of ADHD – show pronounced symptoms of EFA deficiency. Children with lower n-3 fatty acid concentrations and more pronounced physical symptoms of EFA deficiency also suffer from behavioural disorders, hyperactivity-impulsiveness, anxiety, fits of rage, difficulties in falling asleep, and learning disorders. Stevens et al. therefore concluded that omega-3 acids are more important for the brain function, behaviour and learning [32].
Many other studies with numerous confounding factors have been conducted on both humans and animals, but they do not indicate consistent positive effects; the only thing they do confirm is that breastfeeding affects the development of intelligence and sight function. Following the recent increase in incidental illnesses of an allergic nature, interesting studies have examined the potential role of polyunsaturated fatty acids in preventing allergies. One of them is Dustan’s study which encompassed 93 pregnant women who consumed fish oil for 20 weeks of pregnancy until delivery. Results show that their children had higher PUFA levels in erythrocyte membranes and a lower concentration of neonatal cytokine compared to the control group. During their first year of life, this group of infants was 3 times less likely to get positive results on the skin prick test for nutritive allergens. Unfortunately, the frequency of atopic dermatitis remained the same [33].
Several studies point to a significant positive correlation between DHA and the perception of speech performance. At the age of 2 months, infants with higher DHA blood levels are more frequently able to differentiate between phonetic syllables in languages other than their mother tongue; at the age of 6 to 8 months, they were able to differentiate syllables of their mother tongue more frequently than those of foreign languages [34]. However, few published studies address the development of speech and hearing, making it difficult to deduce whether the immediate benefits of DHA consumption do in fact exist.
One might conclude that brain development is a complex, interactive process, and that potential harmful effects that appear during intensive initial development can cause long-lasting consequences on later development and functional adaptations.
Koletzko reports on recommendations prepared by the Perinatal Lipid Intake Working Group, based on the findings presented above [35]. Recommended dietary fat intake for pregnant and breastfeeding women (as part of the overall energy intake) is the same as the recommended intake for the general population. Pregnant and breastfeeding women should aim for a minimum intake of 200 mg/day omega-3 fatty acids to supply DHA. In experiments, the daily intake of 1g of DHA to 2.7g of omega-3 fatty acids did not show any significant side effects [35]. Women of fertile age can meet the daily recommended DHA intake requirements by consuming 1–2 portions of fish a week, including oily fish. The choice of fish should cover a wide variety of species, but larger predatory fish should be avoided due to the increased risk of methylmercury poisoning. Precursor intake in ALA synthesis is less efficient in developing brain function than the intake of already processed DHA. Similarly, women who consume LA do not have to consume AA. Monitoring the diet of pregnant women and providing them with advice on possible dietary anomalies should begin as early as the first trimester. Diet in the preconception period and during pregnancy should include folic acid, as it reduces the risk of neural tube defects (anencephaly and spina bifida). Furthermore, larger amounts of folic acid (600 micrograms) are needed during the first month of gestation to prevent Down syndrome. Authors of the study [36] also reached the conclusion that the simultaneous consumption of folic acid and fatty acids increases DHA and EPA levels in maternal blood. As far as infant nutrition is concerned, breastfeeding (provided that the mother is receiving proper, healthy nutrition recommended for breastfeeding women) remains the best choice. Authors of the study [37] which examined the guidelines provided by the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) and the Codex Standard for Infant Formula adopted by the Codex Alimentarius Commission of the Food and Agriculture Organization of the United Nations present the following conclusions: infant formula should be supplemented with DHA and AA; DHA should assume a minimum value of 0.2% fatty acids and a maximum value of 0.5%; the amount of supplemented AA should be at least equal to the amount of supplemented DHA, while the amount of supplemented EPA should not exceed the amount of supplemented DHA; LCPUFA supplements should continually be added to infant food during the second half of infancy (6–12 months); intensive brain development continues during early childhood, so it is necessary to introduce LCPUFA-rich complementary foods (e.g. eggs, oily fish, meat and highly refined olive oil); specific requirements for the development of older children are not known; during preschool years, the child’s DHA requirements are met via nutrition rich in omega-3 fatty acids and zinc; sea food stimulates brain development because it is rich in DHA, as well as iodine, taurine and zinc; DHA levels in animal milk, meat, poultry and eggs can be increased by feeding the animals and poultry omega-3-rich food; it has been proven that eggs laid by chickens fed with flax fibres or microalgae are full of DHA (up to 150 mg per egg) [9].
Recent decades have seen extensive research into the role of LCPUFA in regulating gene expression, considering the potential of dietary fatty acids to influence several developmental and metabolic processes with appropriate short-term and long-term health effects [38, 39, 40, 41]. The mechanism that regulates gene expression via fatty acids includes members of the nuclear receptor super family, which function as transcription factors. It is hoped that understanding how fatty acids regulate transcription factors that play a significant role in carbohydrate and lipid metabolisms will create opportunities for developing nutritionist interventions and therapeutical strategies to potentially influence several chronic illnesses such as coronary heart disease and atherosclerosis, obesity, Type II diabetes, major depression disorders and schizophrenia [42].
Based on these findings, it is necessary to highlight the public health importance of this problem, the need to organise a wide–ranging initiative aimed at educating the public on the effects of essential fatty acids on childhood growth and development, as well as the importance of healthy nutrition during pregnancy and early childhood in general.
Figure 1
DHA concentration in maternal blood during pregnancy and the postpartal period
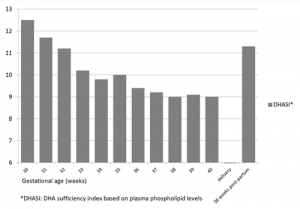
DHASI= DHA sufficiency index based on plasma phospholipid levels
References:
- Karlson P. Biokemija, VIII. izdanje prema XIII. njemačkom izdanju, Zagreb: Školska knjiga; 1993: 256-8.
- Clandinin MT, Jumpsen J, Suh M. Relationship between fatty acid accretion, membrane composition and biologic function. J Pediatr 1994; 125(5): 25-32.
- British Nutrition Foundation Task Force. Unsaturated fatty acids, nutritional and physiological significance. The report of BNF task Force, London: British Nutrition Foundation,1992.
- Pawlosky RJ, Hibbelin JR, Novotny JA, Selem N. Psychological compartmental analysis of linolenic acid metabolism in adult humans. J Lipid Res 2001;42:1257-65.
- Mayers PA. Metabolism of unsaturated fatty acid and eicosanoids. In: Murray RK, Granner DK, Mayers PA, Rodwell VW, eds. Harper s Biochemistry 24th edn. Prentice Hall London 1996;236-44.
- Haag M. Essential fatty acid and the brain. Canad J. Psychiatry 2003; 48: 195-203.
- Singh M . Nutrition, brain and environment. How to have smarter babies? Indian Pediatr 2003;40: 213-20.
- Ghafornissa SA. Requirements of dietary fats to meet nutritional needs and prevent risk of atherosclerosis: an Indian perspective. Indian J Med Res 1998; 108: 191-202.
- Singh M. Essential fatty acids, DHA and human brain. Indian J Pediatr 2005;72(3):239-42.
- Clandinin MT, Chappel JE, Leong S, Heim T, Swyer PR, Chance GW. Intrauterine fatty acid accretion in human brain: implications for fatty acid requirements. Early Hum Dev 1980; 4:121-29.
- Uauy R, Mena P, Rojas C. Essential fatty acids in early life: Structural and functional role. Proceedings of the Nutrition Society 2000; 59: 3-15.
- Smuts CM, Huang M, Mundy D, et al. A randomized trail docosahexaenoic acid supplementation during the third trimester of pregnancy. Obstet. Gynecol 2003; 101(3): 469-79.
- . Fidler N, Sauerwald T, Pohl A et al. Docosahexaenoic acid transfer into human milk after dietary supplementation: a randomized clinical trial. J Lipid Res 2000; 41: 1376-83.
- Makrides M, Neuman MA, Gibson RA. Effects of maternal docosahexaenoic acid (DHA) supplementation on breast milk compositions. Euro J Clin Nutr 1996;50: 352-7.
- Burgess JR, Stevens L, Zhang W, Peck L. Long chain polyunsaturated fatty acids in children with attention deficit hyperactivity disorder. Am J Clin Nutr 2000;71(1):327-30.
- . Lauritzen L, Hansen HS, Jorgansen MH, Michaelsen KF. The essentiality of long chain n-3 fatty acids in relation to develop and function of the brain and retina. Prog Lipid Res 2001;40:1-94.
- . Michaelsen KF, Lauritzen L, Jorgensen MH, Martenson EL. Breast feeding and brain development. Scandinavian Journal of Nutrition 2003; 47(3):147-51.
- Mortensen EL, Michaelsen KF, Sanders SA, Reinisch JM. The association between duration breastfeeding and adult intelligence. JAMA 2002;287:2365-71.
- Anderson JW, Johnstone BM, Remely DT. Breast-feeding and cognitive development: a meta-analysis. Am J Clin Nutr 1999;70: 525-35.
- Drane DL, Logemann JA. A critical evaluation of the evidence of the association between type of infant feeding and cognitive development. Pediatr Perinat Epidemiol 2000; 14: 349-5.
- Bouwstra H, Dijck-Brouwer DA, Wildeman JA, et al. Long-chain polyunsaturated fatty acids have a positive effect on the quality of general movements of healthy term infants. Am J Clin Nutr 2003;78:313–8.
- Dziechciarz P, Horvath A, Szajewska H. Effects of n-3 long-chain polyunsaturated fatty acid supplementation during pregnancy and/or lactation on neurodevelopment and visual function in children: a systematic review of randomized controlled trails. J Am Coll Nutr 2010; 29: 443-54.
- Gjurić G. Prehrana. U: Mardešić i sur. Pedijatrija, 7 izdanje, Zagreb: Školska knjiga; 2003:231-303.
- Badart Smook A, van Houwellingen AC, Ai MDM, et al. Fetal growth is associated positively with maternal intake of riboflavin and negatively with maternal intake of linolenic acid. J Am Diet Assoc 1997; 97: 867-70.
- Rump P, Hornistra G. The n-3 and n-6 polyunsaturated fatty acid composition of plasma phospholipids in pregnant women and their infants. Relation with maternal linolenic acid intake. Clin Chem Lab Med 2002; 40: 32-9.
- Hornstra G. Importance of polyunsaturated fatty acids of the n-6 and n-3 families for early human development. Eur Lipid Sci Technol 2001;102:379-89.
- Honstra G. Essential fatty acids during pregnancy, Impact on mother and child. Nestle Nutrition Workshop Series Pediatric Program, The Impact of Maternal Nutrition on the Offspring 2005, 55:83-96.
- Horvath A, Koletzko B, Szajevska H. Effect of supplementation of women in high-risk pregnancies with long-chain polyunsaturated fatty acids on pregnancies outcomes and growth measures at birth: a meta-analysis of randomised controlled trials. Br J Nutr 2007;98:253-9.
- Szajewska H, Horvath A, Koletsko B. Effect on n-3 long chain polyunsaturated fatty acid supplementation of women with low-risk pregnancies on pregnancy outcomes and growth measures at birth: a meta-analysis of randomized controlled trails. Am J Clin Nutr 2006; 83:1337-44.
- Jensen CL, Voigt RG, Prager TC, Llorente AM, Peters SU, Prager TC, Zou YL, Rozelle JC, Turcich MR, Fraley JK, Anderson RE, Heird WC. Effects of early maternal docosahexaenoic acid intake on neuropsychological status and visual acuity at five years of age of breast-fed term infants. J Pediatr 2010; 157 (6):900-5.
- Stevens LJ, Zentall SS, Deck JL, et al. Essential fatty acid metabolism in boys with attention- deficit hyperactivity disorder. Am J Clin Nutr 1995; 62:761-8.
- Stevens LJ, Zentall SS, Abate ML, Kuczek T, Burgess JR. Omega-3 fatty acids in boys with behavior, learning and health problems. Psyhol Behav 1996; 59:915-20.
- Dunstan JA, Mori TA, Barden A, Beilin LJ, Taylor AL, Holt PG, Prescott SL. Fish oil supplementation in pregnancy modifies neonatal allergen-specific immune responses and clinical outcomes in infants at high risk of atopy: a randomized, controlled trail. J Allergy Clin Immunol 2003;112(6):1178-84.
- Innis SM, Gilley J, Werker J. Are human milk long-chain polyunsaturated fatty acids related to visual and neural development in breast-fed term infants? J Pediatr 2001; 139(4):532-8.
- Koletzko B, Cetin I, Brenna J, for the Perinatal Lipid Intake Working Group. Dietary fat intake for pregnant and lactating women. Br J Nutr. 2007;98:873-8.
- Krauss-Etschmann S, Shadid R, Campoy C, Hoster E, Demmelmair H, Jimenez M, Gil A, Rivero M, Veszpremi B, Decsi T, Koletzko BV for the NUHEAL Study Group. Effects of fish-oil and folate supplementation of pregnant women on maternal and fetal plasma concentrations of docosahexaenoic acid and eicosapentaenoic acid: a European randomized multicenter trial. Am J Clin Nutr 2007; 85:1392-400.
- Koletzko B, Lien E, Agostoni C, Bohles H, Campoy C, Cetin I, Decsi T, Dudenhausen JW, Dupont C, Forsyth S, Hoesli I, Holzgreve W, Lapillonne A, Putet G, Secher NJ, Symonds M, Szajewska H, Willatts P, Uauy R. The roles of long-chain polyunsaturated fatty acids in pregnancy, lactation and infancy: review of current knowledge and consensus recommendations. J Perinat Med 2008; 36: 5-14.
- Jump DB. Dietary polyunsaturated fatty acids and regulation gene transcription. Curr Opin Lipidol 2002;13:155-164.
- Jump DB, Thelen A, Ren B, Mater M. Multiple mechanisms for polyunsaturated fatty acid regulation of hepatic gene transcription. Prostaglandins Leukot Essent Fatty Acids 1999;60:345-349.
- Raclot T, Oudart H. Selectivity of fatty acids on lipid metabolism and gene expression. Proc Nutr Soc 1999;58:633-646.
- Clarke SD, Gasperikova D, Nelson C, et al. Fatty acid regulation of gene expression: A genomic explanation of the Mediterranean diet. Ann NY Acad Sci 2002;967:283-98.
- Hertz R, Magenheim J, Berman I, Bar-Tana J. Fatty acil-CoA thioesters and ligands of hepatic nuclear factor 4 alpha. Nature 1998;392:512-16.




